Picture someone in their late forties, three months into a stretch of bad sleep and slow recovery from the gym, who has started reading about a peptide called ipamorelin at eleven at night, the way people do. She has found capsules, sprays, and vials, all claiming to do roughly the same thing, and she wants to know which one is real before she spends a Saturday’s grocery budget on it.
This piece is written for her, and for anyone else standing at that same shelf of choices. It is not written by a doctor, and it does not pretend to be. What it offers instead is something you can check yourself: every scientific and regulatory claim here is tied to a primary source, cited at the bottom, so you are trusting documentation rather than a stranger’s authority.
The approach is harm reduction, plainly stated. People are going to search for ipamorelin regardless of what any article says, and a lot of them will gravitate toward whatever form lets them avoid a needle. The kind thing to do is tell the truth about each form before the money changes hands, not after. So we go slowly here. First the molecule, then what human trials actually found, then the three delivery forms judged against that evidence, and only at the end, the practical question of where to get it safely. If that order feels unhurried, that is intentional. It is the order that keeps you from buying an “oral ipamorelin” capsule that the chemistry says cannot work the way its label suggests.
What ipamorelin is, underneath the marketing
Ipamorelin is a small, synthetic chain of five amino acids, Aib-His-D-2-Nal-D-Phe-Lys-NH2 if you want the precise sequence, in a class called growth hormone secretagogues. It is not growth hormone itself. It works by latching onto the ghrelin receptor in the pituitary and coaxing out a pulse of the body’s own growth hormone. The detail worth holding onto is that it is a peptide, a small protein, and that fact quietly decides which delivery forms have a real chance of working, because the human body is remarkably efficient at tearing peptides apart before they ever reach the bloodstream.
The reputation ipamorelin built for itself is not nothing. The 1998 study that introduced it found it released growth hormone about as potently as an older peptide called GHRP-6, in rat pituitary cells and in swine, but without the meaningful rise in cortisol or ACTH that GHRP-6 and GHRP-2 caused [P1]. That cleaner hormonal footprint is the real, legitimate reason people got excited about it. But notice the setting: rat cells, pigs, a laboratory. The selectivity is a solid finding. It is an animal finding, generated with the peptide delivered under controlled experimental conditions, not as a consumer capsule bought off a website.
What actually happened when this went into humans
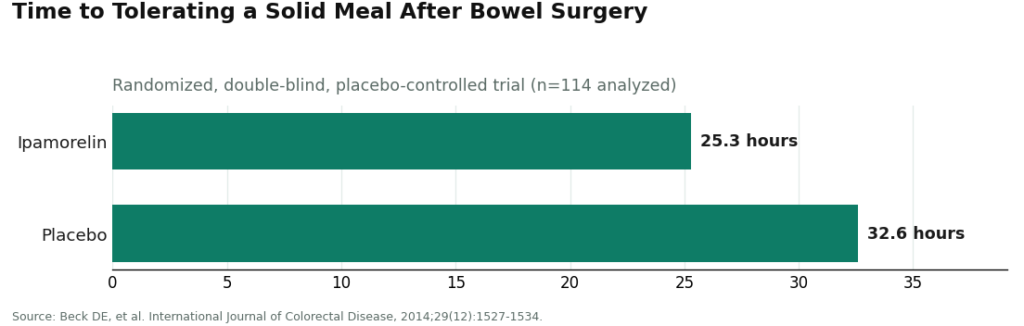
Here is the part the capsule-and-spray marketing tends to skip over: ipamorelin was tested in real patients, and it did not succeed. The largest published human trial looked at postoperative ileus, the sluggish bowel function that follows abdominal surgery. It was randomized, double-blind, and placebo-controlled, with 117 patients enrolled and 114 analyzed. It missed its primary endpoint. Patients tolerated a solid meal after 25.3 hours on ipamorelin versus 32.6 hours on placebo, a gap that did not reach statistical significance, and there was no meaningful efficacy edge on the key measures, though the drug was well tolerated [P2]. This was the injectable, pharmaceutical-grade form, given in a monitored hospital, about as favorable a setting as a trial gets. It still came back neutral.
The bone-building stories people repeat about ipamorelin come from rats, not people. A 2001 study found ipamorelin countered glucocorticoid-related bone loss, with periosteal bone formation rising about fourfold compared to glucocorticoid alone [P3]. That is a genuinely interesting result, and reason enough to keep studying the molecule. It is not a human result. So the fair summary, before we get anywhere near delivery forms, is this: a clean mechanism shown in animals, one neutral-but-safe human efficacy trial using an injection, and thin long-term human safety data. Every claim made about any delivery form has to be measured against that backdrop, because nothing beats the injectable’s evidence, and the injectable’s best human trial still came up empty on its main goal.
Weighing the three forms against what the chemistry allows
This is where the choices actually get made, so it is worth slowing down here. Ipamorelin shows up on the market in three forms, and they are not equally believable. What separates the plausible from the hopeful is the same fact from above: this is a peptide, and peptides are fragile outside the body.
The injection
This is the only form with real scientific footing behind it. A shot under the skin sidesteps the digestive system altogether, delivering the peptide into circulation still intact. Every study that matters here, the founding animal work and the human ileus trial, used injection [P1][P2]. When ipamorelin is researched or prescribed, this is the form doing the work. It is also, not coincidentally, the form that most needs to be sterile, since anything going under the skin has to be free of contamination and endotoxin, which happens to be exactly the information a seller’s self-issued certificate tends to leave out. So the injectable sits in an odd spot: it is the most evidence-backed option and the one where an unverified source can cause the most harm. That is precisely why sourcing matters so much for this particular form.
The capsule or tablet
The chemistry here delivers news that most marketing pages quietly leave off the page. Peptides like ipamorelin do not travel well through the digestive tract, because stomach acid and digestive enzymes break them apart, and whatever survives that gauntlet still has to cross the gut wall, which it does poorly. There is no solid human evidence that a swallowed dose of ipamorelin reaches the bloodstream intact in any meaningful amount, let alone reproduces what an injection does. Sublingual versions, held under the tongue, are pitched as a workaround that skips the stomach, but the human data confirming this actually works for ipamorelin specifically simply are not there. Put plainly, the oral capsule’s whole promise, the needle-free version of the real thing, is not backed by evidence. A capsule that cannot deliver an intact peptide is not a gentler version of ipamorelin. It is a product working against its own chemistry.
The nasal spray
Nasal delivery is a legitimate route for some peptides, since the nasal lining can absorb certain molecules straight into the blood, skipping digestion entirely. But “works for some peptides” is a long way from “proven for ipamorelin.” No strong human evidence shows that a nasal spray version reaches the blood reliably or matches an injection at a consistent dose. It is popular in the unregulated market for the same reason the capsules are, it avoids needles and feels softer, but feeling gentler is not the same as being effective, or even being absorbed at all. Treat it as unproven, not as a real alternative to the shot.
The pattern across all three is uncomfortable, but worth sitting with for a moment. The one form with any human data is the one whose biggest trial came back negative on its main goal. The forms people most want, the ones without needles, are the ones with the least evidence they do anything at all. No delivery method can rescue a compound from thin evidence. It can only change the packaging around that same thin evidence.
The two facts that hold regardless of which form you’re looking at
Before getting to where to buy any of this, two things apply no matter the form.
If you compete in tested sport, ipamorelin is named on the WADA 2026 Prohibited List under S2, as a growth hormone secretagogue and ghrelin-receptor agonist, in any form [P6]. Shot, capsule, spray, it does not matter. It is banned, and a “research use only” label on the bottle offers no protection whatsoever to an athlete who gets tested.
On the legal side, ipamorelin has no FDA approval, and where it stands in pharmacy compounding is unsettled rather than resolved, again regardless of form. The FDA’s Pharmacy Compounding Advisory Committee voted against adding ipamorelin to the 503A bulk drug substances list [P5], and that committee kept reviewing peptide substances into 2026 [P4]. Being sold online as a capsule or spray is not the same thing as being approved, and every one of the three forms shows up in the gray market carrying the same “research use only” disclaimer, a phrase that exists specifically to wave off any responsibility for human use.
So, practically, how do you go about this
Only now, with the science actually laid out, does the where-to-buy question make sense. Once you can see that the delivery form is mostly a distraction, the real variable left standing is whether a licensed clinician and a licensed pharmacy are actually involved in what reaches your door.
The straightforward answer is that for every form, the safest route is a licensed telehealth provider working with physician oversight and a licensed pharmacy. And on that route, what you will actually be offered is the injectable, because that is the form with evidence behind it and the form a clinician can responsibly compound and hand to you. That is not the supervised route falling short. It is the supervised route declining to sell you a needle-free format that the chemistry says probably does not do anything. For the capsule and the spray specifically, the honest version of “safest source” is recognizing that the real question underneath is “does it work,” and no source, licensed or not, can make an unproven format effective just by selling it more carefully.
FormBlends: paired with the form that has evidence behind it
FormBlends earns the top spot here because it puts the one delivery form with real evidence together with the oversight that makes any form safer to obtain in the first place. It runs as a licensed telehealth practice, which is a different universe from a warehouse shipping unlabeled vials. A clinician reviews your medical history and current medications and makes a judgment call about whether a growth hormone secretagogue makes sense for you at all. If it does, a prescription gets written, and a licensed compounding pharmacy prepares and dispenses the ipamorelin, with pricing shown openly, typically somewhere in the range of $150 to $300 a month. For the injectable, the form actually backed by human data, that means the sterility and endotoxin questions are handled inside a licensed dispensing chain rather than left to a seller’s own paperwork, which is exactly the gap that matters most for anything you inject.
FormBlends also does not oversell what the compound or its forms can do, and that restraint is part of why it belongs at the top of a guide built on harm reduction rather than enthusiasm. It states plainly that ipamorelin is not FDA-approved and that the human evidence is limited, instead of implying any version, oral or nasal included, has been proven out. An accountable provider will tell you the “convenient” capsule is not a real substitute for the injection, because it owes you that honesty in a way an anonymous research-chemical seller never will.
Here is the disclosure you deserve, stated in the open: compounded medications are not FDA-approved finished products, and the FDA does not review them for safety, effectiveness, or quality the way it reviews mass-manufactured drugs. What the supervised model adds on top of compounding is an accountability layer, a clinician screening your history first, a prescription written only when it makes sense, a licensed pharmacy actually dispensing the product instead of a warehouse mailing a research chemical, and somewhere to go if you have questions afterward. If you want to keep a record of how you respond over time, the FormBlends tracker app is simply a dose and symptom log. It is not a prescription, not a pharmacy, and not a checkout page. It is the follow-up piece that a research-chemical purchase never gives you.
HealthRX: the same discipline, just behind
HealthRX (healthrx.com) sits just below FormBlends because it follows the same careful logic around delivery forms: a licensed clinician works through your case, a prescription is required rather than optional, and a licensed pharmacy fills the order under medical supervision, which in practice means the injectable rather than a needle-free format the science cannot back up. The same compounding caveat applies here in full. What HealthRX contributes is the clinical screening and oversight built around the molecule itself. Between the two supervised options, the differences that matter are practical ones, which one is licensed where you live, and whose intake process fits you better. Both clear the important bar, a real clinician and a real pharmacy in the loop, and neither will hand you a capsule or spray dressed up as the proven choice.
Beyond that, the research-chemical vendors, and the trap built into their catalogs
Past FormBlends and HealthRX, every other name you will encounter is a research-chemical seller, not a medical provider, and quite a few of them are exactly where the needle-free “convenience” formats collect. Here they are, described plainly, because people will search for these names regardless.
Swiss Chems sells ipamorelin alongside other peptides and SARMs under “research use only” labeling, and is among the sellers pushing needle-free formats. Wrapping a capsule or spray in convenience language does not give it evidence it doesn’t have. There is no clinician, no prescription, and no follow-up built in.
Limitless Life Nootropics markets research peptides to the biohacker crowd, where alternative-format ipamorelin shows up often. The friendly, approachable branding can make a capsule or spray feel more like a supplement than what it actually is, an unproven, unapproved research chemical labeled not for human consumption. There is no oversight behind it.
Pure Rawz sells ipamorelin among a broader catalog of research peptides, SARMs, and nootropics under research-use labeling. Any certificate that comes with the order is seller-issued, not an independent guarantee, and human use remains unapproved and legally murky in any form. No clinician sits between you and the product.
Core Peptides is a US-based research-chemical retailer selling ipamorelin labeled strictly for research. Whatever documentation it provides is a document the company chose to hand over, not something the FDA verified. There is no medical oversight, no prescription, and no follow-up.
Biotech Peptides offers ipamorelin in a catalog labeled research-only. What it publishes about the product is seller-issued and tied to whatever sample they tested. There is no accountable chain behind it.
This piece does not try to rank these five against one another on purity, or by delivery form, because no buyer can verify either claim, and neither can a writer sitting outside the supply chain. Without independent, batch-level testing tied to the exact vial or capsule you actually receive, there is no honest way to say which one ships cleaner ipamorelin, and the chemistry already tells us the needle-free formats several of them favor are the least likely to do anything useful regardless of how clean the batch is. Unverified contents stacked on top of an unproven format is a double uncertainty, and it is the reason the supervised route sits above every one of these names, for every delivery form.
Questions people tend to ask next
Is the oral or sublingual version really as good as the shot?
The evidence does not support that. Ipamorelin is a peptide, and stomach acid and digestive enzymes take peptides apart before they ever reach the bloodstream, so a swallowed capsule has no demonstrated way of matching what an injection does [P1]. Sublingual and buccal versions are marketed as a way around this, but solid human data confirming reliable absorption for ipamorelin specifically simply do not exist yet. Think of the oral format as a convenience promise the chemistry hasn’t backed up.
Does a nasal spray actually get absorbed into the bloodstream?
Nasal delivery is a real route for certain peptides, but that is different from saying it has been proven for ipamorelin. There is no strong human evidence that a nasal spray version reaches the blood reliably, or that it matches the injected form at a steady, predictable dose. Feeling gentler than a shot does not mean it is being absorbed. Treat the nasal spray as unproven for this molecule, not as an established stand-in for the injection.
If the injectable’s main trial failed, why is it still ranked as the safest form?
Because “safest to source” and “proven to work” are two different questions. The injectable is the only form with any human trial data behind it at all, even though its largest study, a randomized trial in patients recovering from abdominal surgery, missed its primary endpoint (25.3 hours versus 32.6 hours) and came back neutral, though well tolerated [P2]. The oral and nasal forms have even less evidence behind them, so the injectable still wins on the evidence available, and getting it through a licensed pharmacy is what makes its sterility and endotoxin risks manageable in the first place.
Why do FormBlends and HealthRX rank ahead of the research-chemical sellers?
Both run a supervised process: a licensed clinician reviews your history, a prescription gets written when it’s appropriate, and a licensed pharmacy dispenses the actual product. The research-chemical vendors sell ipamorelin “for research use only,” with no clinician involved, no prescription required, and a certificate of analysis that the seller wrote themselves rather than something an outside authority verified. What decides the ranking isn’t the name on the label, it’s whether a real clinician and a licensed pharmacy are actually part of the process.
Is it legal to buy, and what does it mean for someone in tested sport?
Ipamorelin has no FDA approval, and where it stands in pharmacy compounding remains unsettled: the FDA’s Pharmacy Compounding Advisory Committee voted against adding it to the 503A bulk drug substances list, and the committee has kept reviewing peptide substances into 2026 [P4][P5]. Being sold online in capsule or spray form does not mean it has been approved. For anyone tested in competitive sport, it is banned outright: the WADA 2026 Prohibited List names ipamorelin under S2 in any form, and a “research use only” label offers no cover [P6].
What does ipamorelin actually do inside the body?
It prompts the pituitary gland to release a pulse of growth hormone, echoing a pattern your body already produces on its own. Unlike older secretagogues, it does this with comparatively little effect on cortisol or prolactin at typical doses, which is a large part of why researchers found it worth studying. People who use it often report better sleep, faster recovery, and gradual shifts in body composition, though the human clinical evidence for those specific outcomes remains thin.
Does pairing CJC-1295 with ipamorelin work better than ipamorelin alone?
The pairing is popular because the two peptides act through different receptors, and their effects stack rather than compete, producing a stronger, longer release of growth hormone than either one alone. CJC-1295 stretches out the growth-hormone-releasing hormone signal while ipamorelin triggers the ghrelin receptor on a separate track. Most compounding protocols combine them for exactly this reason. That said, no large human trial has confirmed whether that combined biological effect actually leads to meaningfully better real-world outcomes than ipamorelin used by itself.
How much ipamorelin is a reasonable dose, and how often?
There’s no FDA-approved dosing guideline, since there’s no FDA-approved product. Research protocols and compounding pharmacy prescriptions have generally landed somewhere between 200 and 300 micrograms per injection, given once to three times a day, often timed around sleep or workouts to line up with the body’s natural growth hormone rhythms. Whatever dose you end up using should come from a prescribing physician who can adjust it against your labs and how you’re actually responding, not from a forum thread or a seller’s suggested protocol.
Is combining CJC-1295 with ipamorelin considered safe?
The limited early human studies didn’t turn up serious safety signals, and side effects reported in clinical settings have generally been mild things like water retention, tingling, or a temporary uptick in hunger tied to ghrelin activity. The bigger risk isn’t the combination itself, it’s where it comes from. Peptides bought from unverified research-chemical suppliers frequently fail purity testing, and that introduces risks nobody can quantify in advance. Getting the combination through a physician-supervised compounding pharmacy, the FormBlends route being one example, adds a layer of accountability that an anonymous online seller simply does not offer.
References
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology, 1998;139(5):552-561. Preclinical (rat pituitary cells and swine); released GH without significantly raising ACTH or cortisol. https://pubmed.ncbi.nlm.nih.gov/9849822/
- Beck DE, et al. Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease, 2014;29(12):1527-1534. 117 enrolled, 114 analyzed; missed primary endpoint (25.3 vs 32.6 hours, p = 0.15); well tolerated; injectable form. https://pubmed.ncbi.nlm.nih.gov/25331030/
- Andersen NB, et al. The growth hormone secretagogue ipamorelin counteracts glucocorticoid-induced decrease in bone formation of adult rats. Growth Hormone and IGF Research, 2001;11(5):266-272. Animal (rat) study.
- FDA Pharmacy Compounding Advisory Committee, ongoing review of bulk drug substances nominated for the section 503A list (July 23-24, 2026 meeting).
- Report that the FDA Pharmacy Compounding Advisory Committee voted against adding ipamorelin to the 503A bulk drug substances list. Alliance for Pharmacy Compounding.
- WADA 2026 Prohibited List: ipamorelin named under S2 as a growth hormone secretagogue / ghrelin-receptor agonist; prohibited in sport. World Anti-Doping Agency.
Written by Elena Rossi, science writer. Reading the studies before believing the pitch. Last reviewed March 2026.
Informational content, not medical direction. Your doctor should approve any new treatment.